Molina Appeal Form - A written confirmation of receipt of. You, your approved representative (this can be a friend,. Thank you for using the molina healthcare member grievance & appeal process. Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. To make an appeal, you must contact molina within 60 calendar days of the denial. Providers can search and locate the adjudicated. If you are unhappy with the steps we and/or your doctor took for your. Your appeal file includes all of. Grievance we will send appeal suite department to your request.
Return molina healthcare this completed form to: Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. Thank you for using the molina healthcare member grievance & appeal process. Providers can search and locate the adjudicated. A written confirmation of receipt of. Your appeal file includes all of. To make an appeal, you must contact molina within 60 calendar days of the denial. Grievance we will send appeal suite department to your request. You, your approved representative (this can be a friend,. If you are unhappy with the steps we and/or your doctor took for your.
Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. Your appeal file includes all of. Grievance we will send appeal suite department to your request. Return molina healthcare this completed form to: To make an appeal, you must contact molina within 60 calendar days of the denial. You, your approved representative (this can be a friend,. A written confirmation of receipt of. Thank you for using the molina healthcare member grievance & appeal process. If you are unhappy with the steps we and/or your doctor took for your. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process.

Molina Dispute Form PDF Fax Medicare (United States)
You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. Grievance we will send appeal suite department to your request. Return molina healthcare this completed form to: If you are unhappy with the steps we and/or your doctor took for your. To make an appeal, you must contact.
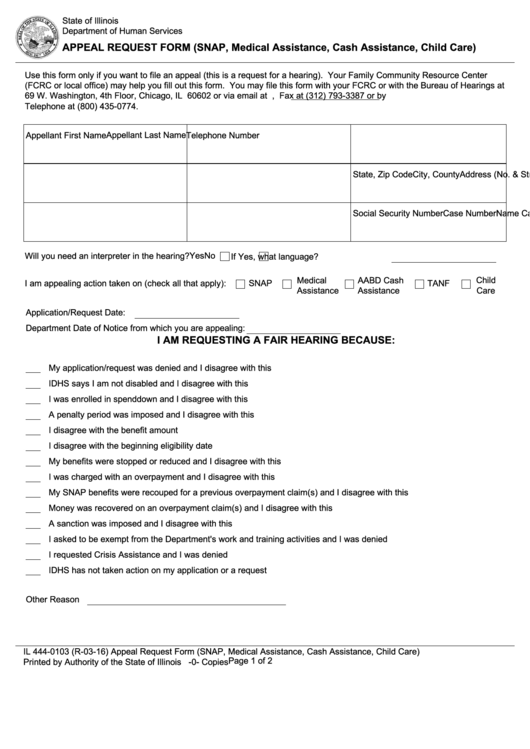
Fillable Appeal Request Form printable pdf download
Return molina healthcare this completed form to: A written confirmation of receipt of. To make an appeal, you must contact molina within 60 calendar days of the denial. If you are unhappy with the steps we and/or your doctor took for your. Grievance we will send appeal suite department to your request.
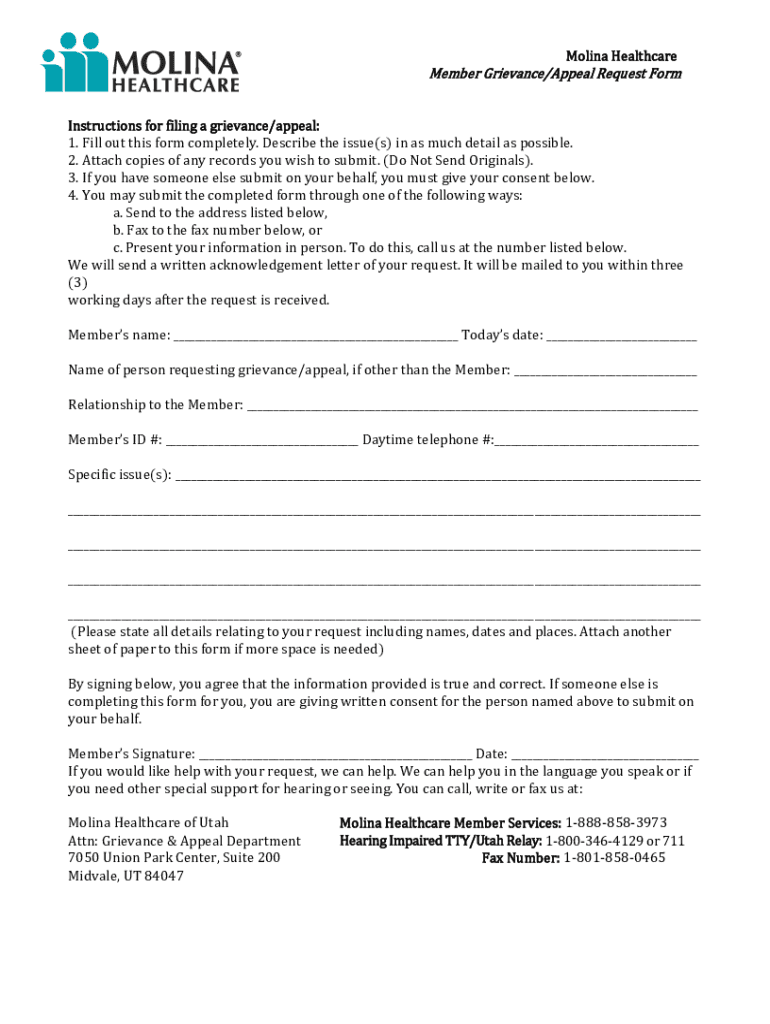
Fillable Online Molina Healthcare Member Grievance/Appeal Request Form
Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. You, your approved representative (this can be a friend,. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. Providers can search and locate the adjudicated. Return molina healthcare this completed form to:

Appeal Form Template
Grievance we will send appeal suite department to your request. A written confirmation of receipt of. If you are unhappy with the steps we and/or your doctor took for your. You, your approved representative (this can be a friend,. To make an appeal, you must contact molina within 60 calendar days of the denial.
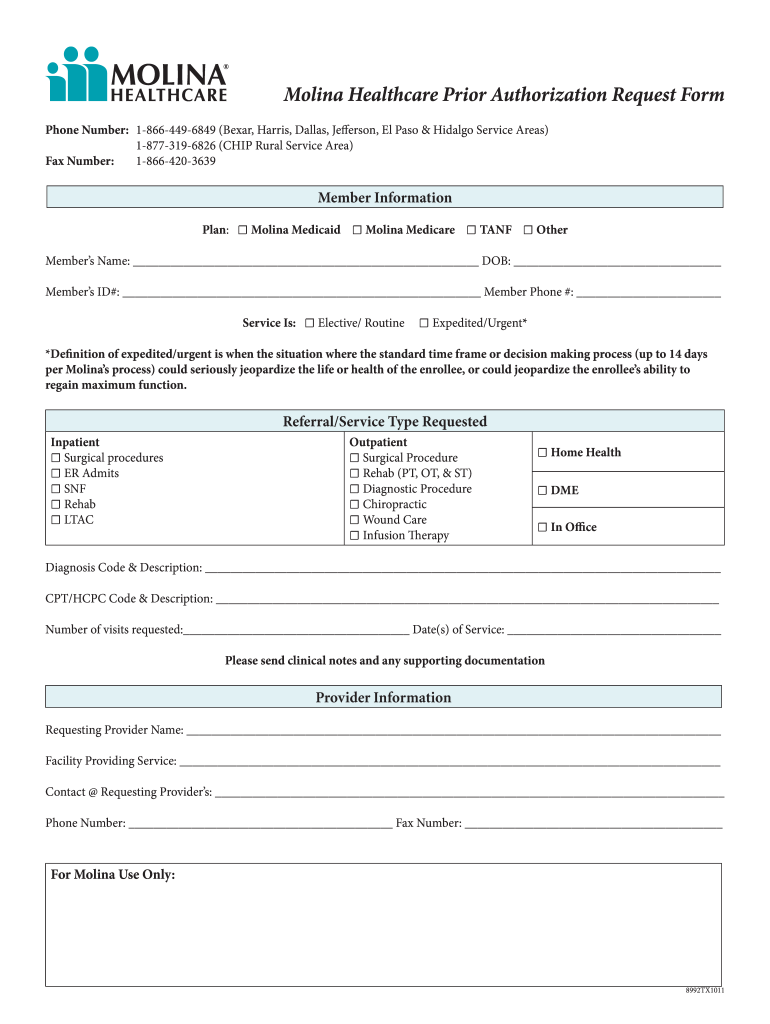
Molina Prior Authorization Pdf Fill Online, Printable, Fillable
A written confirmation of receipt of. Grievance we will send appeal suite department to your request. You, your approved representative (this can be a friend,. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. Return molina healthcare this completed form to:
Molina appeal form Fill out & sign online DocHub
You, your approved representative (this can be a friend,. Grievance we will send appeal suite department to your request. A written confirmation of receipt of. Providers can search and locate the adjudicated. If you are unhappy with the steps we and/or your doctor took for your.
Fillable Online Member GrievanceAppeal Request Form Molina Healthcare
Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. Thank you for using the molina healthcare member grievance & appeal process. You, your approved representative (this can be a friend,. Your appeal file includes all of. To make an appeal, you must contact molina within 60 calendar days of the denial.

Top United Healthcare Appeal Form Templates Free To Download In PDF
Thank you for using the molina healthcare member grievance & appeal process. Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. Your appeal file includes all of. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. Return molina healthcare this completed form.
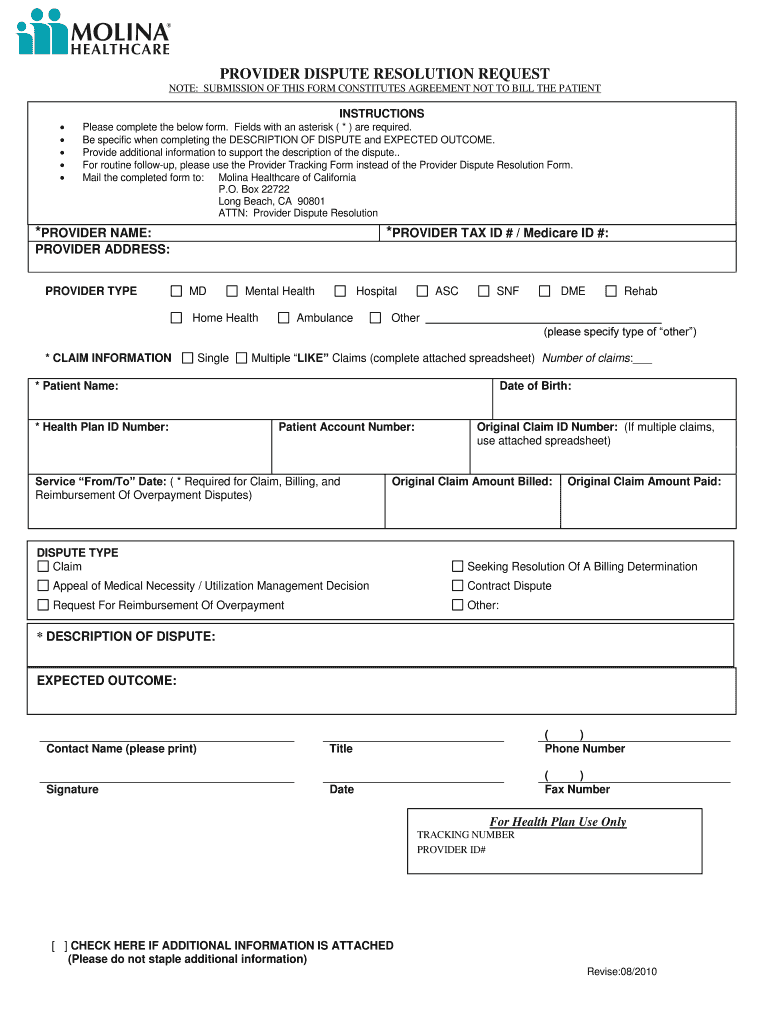
Fillable Online Provider Claim Appeal and Dispute Form Molina
Thank you for using the molina healthcare member grievance & appeal process. Grievance we will send appeal suite department to your request. You, your approved representative (this can be a friend,. Return molina healthcare this completed form to: If you are unhappy with the steps we and/or your doctor took for your.

UT Molina Healthcare Prior Authorization Form 20162022 Fill and Sign
Thank you for using the molina healthcare member grievance & appeal process. Return molina healthcare this completed form to: Grievance we will send appeal suite department to your request. To make an appeal, you must contact molina within 60 calendar days of the denial. If you are unhappy with the steps we and/or your doctor took for your.
Providers Can Search And Locate The Adjudicated.
You, your approved representative (this can be a friend,. To make an appeal, you must contact molina within 60 calendar days of the denial. Grievance we will send appeal suite department to your request. Your appeal file includes all of.
A Written Confirmation Of Receipt Of.
Thank you for using the molina healthcare member grievance & appeal process. You, and/or someone you have chosen to act on your behalf, can review your appeal file before or during the appeal process. Most preferred and efficient method to submit a dispute/appeal is through molina’s provider portal. If you are unhappy with the steps we and/or your doctor took for your.